Whole body vibration therapy with exercise enhances motor function and improves quality of life in Parkinson’s disease
Thursday, June 23, 2016
O.K. Gruder, D.Y. Edmonston, G.Q. Barr, C.G. Maitland (Tallahassee, FL, USA); Meeting: 20th International Congress;
Abstract Number: 2021
Objective: To evaluate the short term effects of whole body vibration and exercise in patients with Parkinson’s disease on overall quality of life, gait, tremor, and postural instability using the GAITRite®System (CRI Systems Incorporated), Unified Parkinson’s disease Rating Scale (UPDRS parts 2,3), Beck Depression Inventory, Fatigue Symptom Inventory (FSI), and Healthy Days Measure (HRQOL-14).
Background: Pharmacologic intervention is the current standard of care for Parkinson’s disease (PD), yet medications frequently fail to control some symptoms, including tremor and postural instability, which degrade functional performance and quality of life. Non-pharmacological treatments, including Whole Body Vibration (WBV) and exercise therapy may reduce these symptoms. We combined basic exercise therapy with WBV in a six-week treatment regimen in order to evaluate their effect on symptoms and signs of PD, with careful attention to postural stability, gait, as well as quality of life measures.
Methods: 15 participants diagnosed with PD (stages 1-4) underwent 12 sessions of WBV combined with exercise therapy over 6 weeks.
| Patients’ Demographics and Characteristics | |||||
| Participant No. | Gender | Age (Years) | Previous Level of Physical Activity* | Pertinent PmHx** | H & Y Staging (UPDRS Motor Score) |
| P01 | F | 74 | Sedentary | Titanium rod in left femur, spinal stenosis | 1-3 |
| P02 | M | 79 | Sedentary | Total knee replacement in right knee | 4 |
| P03 | M | 79 | Moderate Physical Activity | 1-3 | |
| P04 | F | 72 | Sedentary | 4 | |
| P05 | M | 69 | Moderate Physical Activity | 1-3 | |
| P06 | M | 83 | Sedentary | 1-3 | |
| P07 | F | 75 | Moderate Physical Activity | 1-3 | |
| P08 | F | Moderate Physical Activity | 1-3 | ||
| P09 | F | 66 | Vigorous Physical Activity | Previously broken left foot | 1-3 |
| P10 | F | 59 | Sedentary | Untreated torn rotator cuff, osteoporosis, sciatica | 1-3 |
| P11 | F | Sedentary | Arthritic right knee | 1-3 | |
| P12 | M | 77 | Moderate Physical Activity | 1-3 | |
| P13 | M | 79 | Moderate Physical Activity | Chronic neck and back pain | 1-3 |
| P14 | F | 69 | Sedentary | Arthritic right knee | 1-3 |
| P15 | F | 77 | Moderate Physical Activity | 1-3 | |
| P16 | M | Sedentary | Compound vertebral fracture, valve replacement | 4 | |
| P17 | F | 58 | Moderate Physical Activity | 1-3 | |
*Level of physical activity were determined using CDC and ACSM guidelines **All surgeries, replacements were at least 6 months prior to enrolling in the study“. The WBV training included a lower body exercise regimen performed on a vibratory platform.
| WBV and Exercise Regimen | ||||
| Week Number | Session Numbers | Exercises | Duration (Seconds) | Frequency (Seconds[macr]1) |
| 1 | 1,2 | Squats and lunges (static and dynamic), tandem stance (twice on each side) | 30 | 25 |
| 2 | 3,4 | Squats, lunges and calf raises (static and dynamic), tandem stance (twice on each side) | 45 | 25 |
| 3 | 5,6 | Squats, lunges and calf raises (static and dynamic), tandem stance (twice on each side) | 45 | 30 |
| 4 | 7,8 | Squats, lunges and calf raises (static and dynamic), tandem stance (twice on each side) | 60 | 30 |
| 5 | 9,10 | Squats, lunges and calf raises (static and dynamic), tandem stance (twice on each side) | 60 | 35 |
| 6 | 11,12 | Squats, lunges and calf raises (static and dynamic), tandem stance (twice on each side) | 60 | 35 |
Baseline measurements and 2 follow up data collection sessions (1 and 4 days after the final session) included an evaluation of gait via the GAITRite®System, UPDRS parts 2,3, Beck Depression Inventory, FSI, and HRQOL-14.
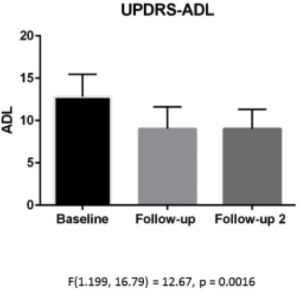
Results: A one-way repeated measures ANOVA was conducted to determine differences between baseline and both post-interventional examinations in all measured parameters. UPDRS scores decreased on average from 29.53(baseline) to 18.00(1 day post-intervention) and 17.53 (4 days post intervention), p<0.001. Both part 2 and 3 of the UPDRS showed statistically significant improvement.

Statistically significant improvement in both post-interventional examination for gait velocity, cadence, and double support time was also observed. No significant difference was observed for FSI, Beck Depression,
Conclusions: WBV combined with exercise therapy has significant effect on motoric performance, ADL related symptoms, and postural stability. This therapy has significant short-term effects.
To cite this abstract in AMA style:
O.K. Gruder, D.Y. Edmonston, G.Q. Barr, C.G. Maitland. Whole body vibration therapy with exercise enhances motor function and improves quality of life in Parkinson’s disease [abstract]. Mov Disord. 2016; 31 (suppl 2). http://www.mdsabstracts.org/abstract/whole-body-vibration-therapy-with-exercise-enhances-motor-function-and-improves-quality-of-life-in-parkinsons-disease/. Accessed September 30, 2016.