Critical Care, DOI 10.1186, 2017; 21/9: 1-10
Whole-body vibration to prevent intensive care unit-acquired weakness: safety, feasibility, and metabolic response
Wollersheim T, Haas K, Wolf S, Mai K, Spies C, Steinhagen-Thiessen E, Wernecke KD, Spranger J, Weber-Carstens S
Department of Anesthesiology and Operative Intensive Care Medicine, Campus Virchow Klinikum and Campus Mitte, Charité—Universitätsmedizin Berlin, Augustenburger Platz 1, Berlin 13353, Germany Berlin Institute of Health (BIH), Berlin 13353, Germany
Abstract
Background: Intensive care unit (ICU)-acquired weakness in critically ill patients is a common and significant complication affecting the course of critical illness. Whole-body vibration is known to be effective muscle training and may be an option in diminishing weakness and muscle wasting. Especially, patients who are immobilized and not available for active physiotherapy may benefit. Until now whole-body vibration was not investigated in mechanically ventilated ICU patients. We investigated the safety, feasibility, and metabolic response of whole-body vibration in critically ill patients.
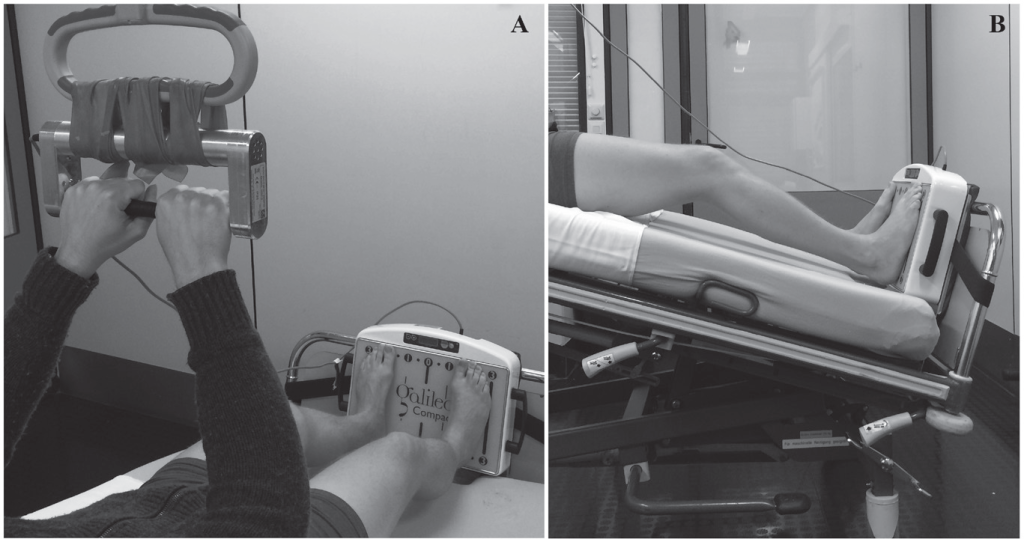
Methods: We investigated 19 mechanically ventilated, immobilized ICU patients. Passive range of motion was performed prior to whole-body vibration therapy held in the supine position for 15 minutes. Continuous monitoring of vital signs, hemodynamics, and energy metabolism, as well as intermittent blood sampling, took place from the start of baseline measurements up to 1 hour post intervention. We performed comparative longitudinal analysis of the phases before, during, and after intervention.
Results: Vital signs and hemodynamic parameters remained stable with only minor changes resulting from the intervention. No application had to be interrupted. We did not observe any adverse event. Whole-body vibration did not significantly and/or clinically change vital signs and hemodynamics. A significant increase in energy expenditure during whole-body vibration could be observed.
Conclusions: In our study the application of whole-body vibration was safe and feasible. The technique leads to increased energy expenditure. This may offer the chance to treat patients in the ICU with whole-body vibration. Further investigations should focus on the efficacy of whole-body vibration in the prevention of ICU-acquired weakness.